In the wake of the January 2025 Los Angeles Wildfires we find ourselves talking a lot about ‘those impacted by the fires.’ But what does it really mean to be impacted? As of today, January 19th, there are 28 confirmed fatalities, 13 confirmed injuries, 1,963 damaged structures and 16,080 destroyed structures between the Palisades Fire and the Eaton Fire. We know that well over 200,000 Angelenos were evacuated during the wildfires. But what do these numbers mean? Certainly they are metrics that can quantitatively tell us that together, this wildfire storm is the second most destructive in California’s history and the third most deadly. But what lies beneath these numbers?
When looking at the activation of FEMA’s individual assistance program, the federal government examines several metrics including the number of structures destroyed. Certainly, the people who have lost their homes in these fires are the most severely impacted next to the families of those who lost their lives. But that is not the end of the story, particularly when fires rage through urban environments decimating entire communities.
Santa Paula playground damaged by the 2017 Thomas Fire.
What about the children who lost their schools and playgrounds to the fires? What about the business owners and patrons who lost their favorite restaurants, grocery stores or retail stores? What about the community members who lost their recreation centers, gyms, or libraries? What about the employees who will lose their jobs as a result of the fire—including laborers such as housekeepers, gardeners, and pool maintenance? Or the renters who will be given notice to vacate because their landlords lost their primary residence and now need to move into their rental property? Or the thousands of first responders who are working around the clock to contain the fires, keep our streets safe, restore power and water, provide shelter, relief and resources to the evacuees?
I would argue that all of the above are impacted by the fires, even if they may not be considered survivors by the metrics. As I wrote about in 2021, we need to broaden the definition of disaster survivors. However, it does not end there. If we pan out we can see that another layer exists—what about the friends and families members of those who lost their homes? What about the friends and family members who took in evacuees during the fires? What about the 500,000 LAUSD children who were kept home from school and their parents who missed work while the entire district closed for the fires? What about the families of the first responders—the children who keep asking why mommy or daddy doesn’t come home for dinner like they used to? What about those throughout the region, particularly those with respiratory conditions, who were forced to alter their routines to stay indoors to avoid toxic ash in the air?
It doesn’t take long to see that major disasters such as the LA wildfires are accompanied by a ripple effect. It is never easy to draw the line between who is impacted and who is not with a disaster of this scale. It has forever changed Los Angeles County and many of its 10 million residents. I believe that nearly all of Southern California is impacted by these fires—it’s just a matter of what shade of grey they fall into. When houses are burning live on local television at 12 o’clock in the afternoon with the firefight crippled by 100 mile per hour winds and when every cell phone in LA County receives a false alarm evacuation alert, wildfire permeates your psyche.
To bear witness to what our community has experienced this January takes its toll. I think that for many of us there is a reluctance to admit that we are impacted. We know that some people have had it much worse. Some people lost everything including their lives in these fires. Those of us who are impacted indirectly are thankful for our health, our families, our homes and our livelihoods. In many cases we don’t believe that we should count as impacted—we feel that donations, the discounts, and mental health support resources should be reserved for those experiencing the darkest shades of grey.
It’s Okay to Not Be Okay
I think it is important to acknowledge the affect of the wildfires and to not be too quick to dismiss the trauma that we have all witnessed. It’s okay to not be okay in times like these. It is okay to call the Employee Assistance Program, take a mental health day, or to seek out emotional and psychological support. At the very least give yourself grace—this was not the way that we wanted 2025 to begin. Don’t feel guilty for feeling sadness, feeling pain. Yes it’s true that others may have it worse but you are impacted too and it’s ok to acknowledge that. We are a community on edge right now—with a seemingly endless series of Red Flag Warnings on our horizon.
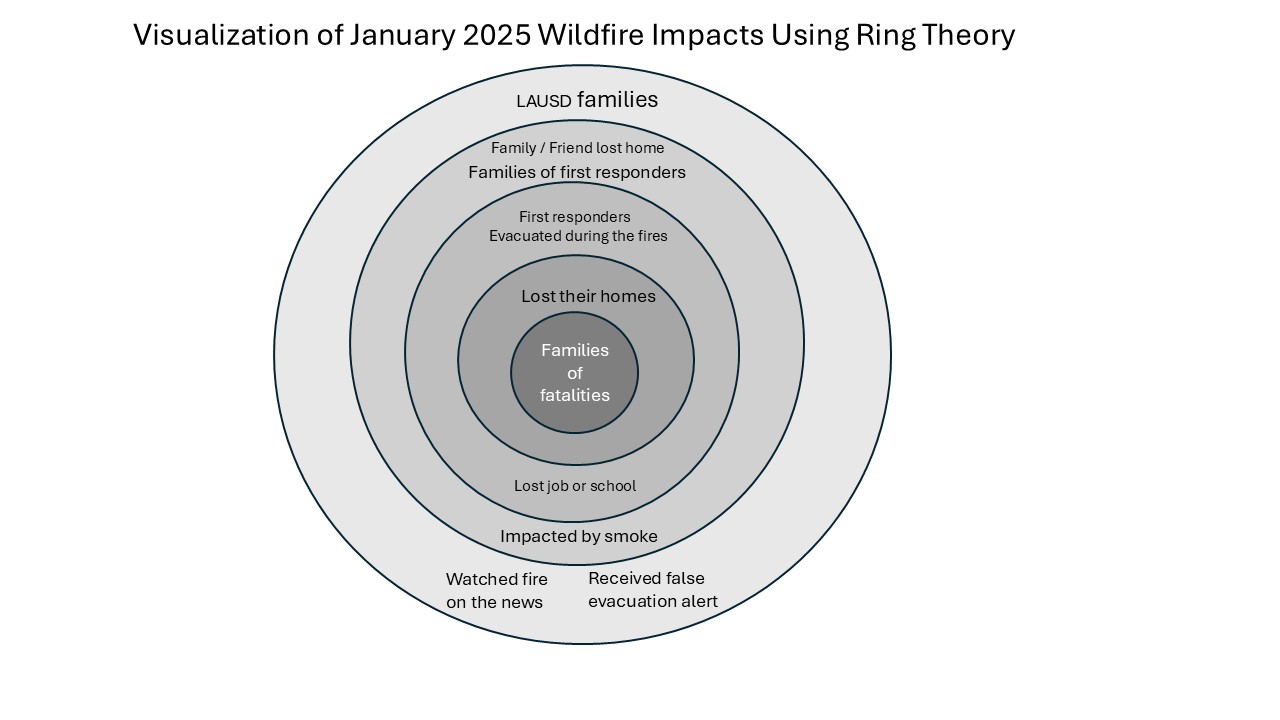
Use the Ring Theory to Give and Seek Support
The Ring Theory paradigm in psychology is used to visualize the ripple effect of a crisis with the most affected individual in the center surrounded by concentric rings with each layer gaining distance from the crisis. We can use this concept to visualize impacts of the LA wildfires and understand how to help. First identify which ring you fall into. As you grapple with your own impacts and trauma from the wildfires, remember to seek support from those who fall in the rings larger than your own but to provide comfort and solace to those who fall in the smaller rings. This will help to ensure that you can find support without placing a greater burden on those who are more heavily impacted than you.
In the early days of a disaster, the media focuses on the event nonstop. The spotlight is shone on the devastated community and an outpouring of physical and monetary donations are given. State and federal resources deploy to support the survivors. They are comforted in shelters, local assistance centers, disaster recovery centers and throughout the community at relief events. But after about 60 days, the world tends to move on. The wildfires will no longer be a daily story, many FEMA resources will be released, and the donations will diminish to a trickle. This is a very critical time for survivors as it is when the finality of the situation sinks in. Everyone else is moving on but they cannot. Recovery is a very long term process and they will begin to feel alone and disheartened. It’s at this time that some survivors will have a better understanding of their trajectory and what their true needs are. Continue to provide support to friends and family who are impacted by checking in, asking about their needs and donating to wildfire relief organizations during this critical time.
It will undoubtedly be a long and rocky road to recovery in the Palisades and Altadena. The most important thing we can do right now is to acknowledge our impacts, recognize where they fall in the rings, and to plan to be there for our fellow Angelenos in the long haul.
Sasha Mae Brown was born via scheduled C-section on Wednesday, August 11th, 2021. Scheduled C-sections typically lend themselves to routine and uneventful birth stories. It could be as simple as selecting a date on a calendar, counting down the days, packing your bags and having a baby. However, Sasha’s birth story was anything but simple.
Sasha’s older sister Scarlett was born during the summer of 2019 after a failed induction. With Scarlett I did not want to be induced, but was pressured into it by my healthcare providers. I have chronic hypertension and best practice is to induce at 39 weeks. Many physicians would try to induce sooner than that. I pushed back as much as I could, convincing my provider to schedule the induction for 40 weeks and 1 day. After days of labor that culminated in nearly 4 hours of pushing, we went into the operating room to deliver Scarlett via C-section. It was a difficult recovery, since I had essentially had the worst of both worlds–the physical pain of labor, prolonged pushing and then the surgery on top of it. It was not a scenario I wanted to repeat and I couldn’t help but think that she was just not ready. If we had not induced so soon Scarlett could have made her debut naturally and would have been much more willing to descend if she had initiated the birth.
I got pregnant with Sasha at 15 months postpartum. My first birth was still quite fresh in mind, so I wanted to avoid induction at all costs with my second child. My goal was to go into labor spontaneously and to have a successful VBAC (Vaginal Birth After Cesarean). From the very beginning, I received pushback from the slew of different OBGYNs I saw at Kaiser throughout my prenatal care. I was surprised by this, given the high success rates of VBACs and that Kaiser seemed to promote vaginal deliveries as the best option in nearly any scenario during the childbirth courses we had taken two years earlier. Yet here I was running into multiple roadblocks and skeptical faces as I tried to advocate early and often for the birth that I wanted.
In my second semester, I switched back to the South Bay / Harbor City hospital where I had delivered Scarlett. A pregnant friend recommended the OBGYN and midwife she was seeing there, telling me that they were not pushy about setting any induction date for her.
I also enlisted the help of a Doula, knowing that success rates are higher for women who have additional support from a Doula. Meredith was great–she met with us in person three times before the delivery. She helped me feel ready mentally and encouraged me to relax.
Our babymoon in Maui
JB and I took a babymoon to Maui over Memorial Day weekend and while I was trying to relax and enjoy the sunshine, I received a phone call from my OBGYN on a holiday. Since it was a holiday, I answered to make sure it wasn’t something urgent. She told me she was reviewing the notes from my first delivery and that the doctor who performed the C-section wrote in the notes that I had CPD (Cephalopelvic distortion), which essentially means that my pelvis was too small for delivery. I was never told that verbally, and through the help of my doula I had been well educated about the myths surrounding CPD and the rarity of true CPD. My doctor told me that she was now recommending that I change my birth plan from a VBAC to a scheduled C-section, stating that she didn’t want me to go through a long labor just to fail in the second stage again.
Although the conversation plucked me straight out of vacation mode and into fits of tears, I told her as best I could that I wanted to stick with my plan. I was well informed of my options and was choosing to pursue VBAC.
As my due date of August 4th loomed nearer, Kaiser started turning up the pressure to get a date on the calendar. They wanted to either induce me or schedule a C-section. The time came for the doctor to let me know that my chronic hypertension meant I should get this date on the calendar for no later than my 40 week due date: August 4th. Prepared for this, I politely declined. I was firm that I did not want an induction. While I really didn’t want to feel the calendar crunch, I understood that I was going to have to make a choice if the baby didn’t come. With my knowledge that the ideal timeframe for birth is 39-41 weeks for healthy pregnancies, and understanding that I was already in a high enough risk category where professionals recommended delivering earlier, I decided I wasn’t comfortable going past 41 weeks. So I would either need to schedule a C-section for August 11th or schedule an induction for a few days earlier if I wanted her out by 41 weeks. I knew I wanted to give the baby as much time as possible to initiate labor. I also knew I wanted to avoid a repeat of my first labor experience, which all began with an induction. Considering all these factors, I begrudgingly conceded to scheduling a C-section with my OBGYN for the evening of August 11th, even though I hoped with every fiber of my being that I would not need the appointment.
Since she was my second baby, I also had childcare to consider. My parents were planning to fly down and be in town for Scarlett’s birthday on July 31st and about 2 weeks afterward. I didn’t know if the baby would come early or late, but I knew that she needed to come and we had to be released from the hospital by the time their return flight was scheduled–August 14th.
Sasha’s Birth Announcement photo at 8 days old.
As I drove to my Non-Stress Test appointment on July 27th, just after I picked up my parents from LAX, I started to feel a funny crampy sensation. It seemed to be coming at regular intervals. I was incredibly excited. I had heard so many birth stories where the mom’s body kicks into labor as soon as she has secured childcare for older children. When I arrived at the NST, I was overjoyed to see that the crampy sensation was indeed coinciding with the contractions that the monitors were picking up. At 38 weeks and 6 days, I was thrilled to think that my labor might be starting.
Unfortunately, the contractions subsided later that evening and I could no longer feel them by bedtime. On Friday, July 30th I had my 39 week OBGYN appointment. Once more, she tried to offer me an induction or C-section date for the following week. I declined again as my blood pressure readings had been beautiful, usually in the 110s/high 60s. She performed a cervical check–and revealed some great news, I was already 3 centimeters dilated and about 50% effaced. During my pregnancy with Scarlett, I was only about 1.5 centimeters dilated before the induction and remained there for the first 24 hours or so of labor until I got the epidural. So I was already farther along! I was so excited and we went home that morning with lots of hope. It didn’t seem possible that this baby was going to stay inside for another 12 days!
In the afternoon, we had to return to the hospital for a growth ultrasound. Apparently because of my high risk pregnancy (due to chronic hypertension which was never an issue in either pregnancy), they wanted to make sure the baby was not too small or too big. I was a little leary of the extra exam. They hadn’t required it with my first pregnancy and I had heard many stories about extra exams leading to unnecessary interventions. But I agreed to get the scan done since my doctor really wanted me to.
They were 45 minutes late calling me into the appointment. I was so upset and had nearly got up to leave before they finally called my name and told me it would be quick. The tech was true to his word and told me that the measurements were looking good. I was relieved and glad to get home to my parents and Scarlett, who was anxiously awaiting her favorite Friday night dinner of beans and rice from the local Mexican place on the eve of her 2nd birthday.
Sasha Mae Brown
Saturday, July 31st was Scarlett’s second birthday. We took her to swim lessons in the morning and she had a blast. Everyone was in good spirits. When we got home I put her down for a nap and sat in the room with her while she fell asleep, a common request that she had at that age. I checked my email on my phone and saw the standard Kaiser email indicating that my results from the growth ultrasound were in. I opened the app, expecting to see everything well within normal range. While the measurements looked good, I was shocked to see that the fluid levels were low and highlighted in italics as falling outside the normal range. My heart started racing, as I was worried that this was indeed going to lead me toward the unwanted interventions and recommendations to induce.
Sure enough, labor and delivery called within an hour and told me I needed to come in and get the fluid levels checked again since they were low on Friday’s scan. We were planning to have a small group of friends over in the evening to celebrate Scarlett’s birthday with cupcakes. The big party had been 3 weeks earlier as we knew the risks with making any firm plans so close to a due date.
I grabbed my purse and JB and headed for L&D, telling my parents we’d be back soon—hopefully before Scarlett woke up from her nap.
At Labor & Delivery, I was placed in a triage room and hooked up to the monitors for a Non Stress Test. We waited anxiously, hoping that we could get some attention soon so that we could head home and celebrate Scarlett’s birthday.
When the medical team finally came in, they performed the ultrasound and had some bad news. The fluid levels had decreased since yesterday. However, they explained that it wasn’t an exact science because the measurements could be obscured by the baby’s position. So it was possible that she was blocking their view of the available fluid pockets. But that wasn’t the only problem. They had also measured a heart deceleration while I was hooked up to the monitors. Baby’s heart rate had recovered, but given that I was full term at 39 weeks and high risk, they were recommending that we stay and get induced.
The entire pregnancy the one day that I did not want Sasha to be born on was Scarlett’s birthday. It was already going to be hard enough with birthdays within a week or two, they didn’t need to share the exact day. Plus, I did not want to be induced. We called our doula, who told us the flaws of the fluid measurements and that low fluid levels was not linked to adverse outcomes at full term. She encouraged us to leave, and that’s what we wanted to do too.
It was difficult to make a decision to go Against Medical Advice (AMA) and leave. I was nervous about it as I have been a believer in western medicine since it saved my life in 2012. But I knew what I wanted out of my birth plan, and I knew that I wanted to spend Scarlett’s birthday with her. I wasn’t ready to stay then. At the very least I needed to go home and celebrate Scarlett’s birthday. I asked if they could check my cervical dilation, but they said they would not until I agreed to stay.
She slept through her first Doctor appointment at 10 days old.
We left anyway. I felt a little crazy and rebellious on the drive home but I also felt like I was finally standing up for myself after being pushed around during my first pregnancy. At home, we had cupcakes and sang to our two-year-old. It was a restless night of sleep for me as I worried that my baby might be in danger, maybe without enough fluid, maybe laying on her umbilical cord which could have caused the deceleration detected at the hospital.
They had promised to call us in the morning and let us know when a bed was available. I still wasn’t sure that I even wanted the induction. But after talking it through with Meredith, I felt like I could possibly be induced and have a different outcome. After all, the circumstances of the first time were markedly different. I had hardly been dilated at all and now I was already at a 3. My body remembered how to get to a 10 and it could be easier this time. Maybe just a little bit of Pitocin would push me into labor. But maybe not. Maybe the contractions would be as intense as they had the first time and I would end up with another cascade of interventions and a C-section.
But I had said I would do what I had to to protect my baby, and now it sounded like she might need to come out. Maybe I couldn’t wait as long as I wanted to. I spent the day Sunday trying to psyche myself up for an induction that I had spent my whole pregnancy swearing I wouldn’t get. It was evening, after 5PM before they called to say that a bed would be ready for me at 7PM. We said good-bye to Scarlett and my parents. This time our bags were fully packed and ready to go. We stopped for ice cream on the way then made the familiar drive to Kaiser South Bay as the sun set. It was surreal to know we’d be coming home with a baby. Her birthday would likely be August 2 or 3. She might share her special day with my dad (8/2).
When we arrived, we had to wait. And wait and wait. I called Meredith to let her know we were just waiting and that we wouldn’t need her to come over until the induction actually started, which could be a while. Labor & Delivery was quite busy. I had been told that it was a pandemic baby boom and they had a lot of trouble finding beds for women.
When we were finally admitted into the same triage room as the previous night, we were met with a kind a doctor who performed an ultrasound and checked my dilation. She had some good, but shocking, news. She said that she was seeing plenty of fluid on the ultrasound, baby had several pockets that were sufficient to keep her well protected in the womb. I was also at 3 dilation and even more effaced. The baby’s heartrate was beautiful on the monitor, no decelerations or other signs of stress. My blood pressure was excellent. She told us that we did not have to stay if we didn’t want to. The induction wasn’t medically necessary, although since I was full term she recommended that we stay. She said induction would likely be easier starting from a 3 and that the baby wasn’t going to get any smaller if I decided to wait, which could make for a more difficult delivery.
It was a tough decision. We had all our stuff there. We had said goodbye to Scarlett and promised baby sister upon return. I had spent all day trying to convince myself to go against my original plan even though I knew in my heart I did not want to be induced. But we decided to leave. And this time they didn’t make us sign the AMA paperwork. The doctor had said we were free to go if we wanted to and the baby was doing well. It was quite the roller coaster of events in one weekend. We went home, happy, tired, and hopeful that our baby girl still had time to come on her own. After all, she still had 10 full days until 41 weeks.
On my due date. I was feeling contractions in this picture.
What I hadn’t anticipated was how difficult the ‘days between’ would be. I hit 40 weeks on JB’s birthday, August 4th, a Wednesday. I had some contractions that day which seemed to intensify and I really hoped that it was happening. But once again they fizzled out. After hitting 40 weeks, the countdown was really on. I was officially past my due date and now had to hope that the extra week I had built into my birth plan would make a difference.
Every day that week was excruciating mentally. We waited. And everyday she didn’t come we grew more and more anxious. We knew the clock was ticking down to the scheduled C-section and to my parents departure date.
On Thursday, August 5th we had an appointment with a nurse practitioner. We had intended to go into it changing our minds, choosing to schedule an induction rather than a C-section. I had been thinking a lot about what the doctor said, and Meredith had been working on convincing me too. I could go for it with the induction and likely get different results, starting from a 3.
The nurse practitioner delivered some shocking news. I was now barely a 1 and my cervix was hard, not effaced. She checked me twice as I relayed to her that two different doctors had told me I was a 3 the previous week. She said that was no longer the case. I had regressed. I was numb with the horror of the revelation. I had thought I would be further along. And yet, I had actually regressed. She said that I was not favorable for induction. We took a few minutes to try to decide what to do. In the couple minutes that passed while she stepped out of the room, my pendulum swung back toward the C-section. I didn’t want the same experience as before after receiving this terrible news.
Devastated, we drove home with the C-section still scheduled. It now felt like it was impending quickly. We decided not to tell any family members about the regression, hoping that if we didn’t say it out loud I could will it not be true. I could mentally coax my cervix into opening.
The next few days I did all the induction things. I walked like crazy. Ate spicy foods, dates, pineapple, did sidewalk walking, had sex and even got out the pump to try breast stimulation. Nothing seemed to be working. Now I felt no contractions. I just felt a sinking sense that my baby would not come, even though I desperately clung to each new day as a possibility that I may get to experience the wonderful spontaneity of labor’s onset.
C-section day.
But baby never came, and on Wednesday, August 11th, we drove back to Kaiser for the scheduled C-section. There were contractions on the monitor, but I didn’t want to be checked. They offered an induction but I turned it down, knowing now that I needed to get home and wanted at least a day with my parents in the house to meet the new baby before they had to return home.
The scheduled C-section was a much more calm and routine process compared with the unscheduled one I’d had during labor 2 years earlier. An all female team delivered my baby and at 6:34PM Sasha Mae was born. She was beautiful, with big blue eyes and the slightest mop of white blonde hair crowning her head. For a scheduled c-section, her birth was certainly accompanied by a roller coaster of emotions. But in the end, she was happy and healthy and I was able to be in charge of my birth, making choices for myself right up until the surgery.
The therapy dog who visited me during my one week stay at UCLA Ronald Reagan Hospital in 2012.
There was a day when I thought I might have only 45 minutes to live. That day was April 27, 2012, exactly ten years ago today.
Ten years. When I was 8 years old, the 10 years between me and my 18th birthday seemed like an eternity. Now that I am 36, ten years feels significant but not forever. I suspect that if I make it to 46, these next ten years will seem even shorter than any decade I have experienced yet.
Ten years ago today was the closest brush with death that I have had. Unwillingly, I was forced to face my own mortality. The presumed invincibility and long term outlook of my 20’s ended abruptly that day.
When I was rushed into emergency surgery, I didn’t know what was wrong with me and neither did the doctors. We only knew that my intestines were obstructed by an unknown mass and if I were to live, it had to come out immediately. I was told I would likely wake up with a colostomy bag and asked to sign a form acknowledging death as a risk of the surgery. I was all alone for most of the 45 minutes I had.
When I woke up from surgery, I was colostomy bag free but faced with the prospect of a long recovery and the lingering mystery of the origin of the mass. Later that week I learned that it was a malignant neoplasm–cancer–the exact type still unknown. I was told it was either a sarcoma or a melanoma, not a carcinoma which is by far the most common type (breast cancer, colon cancer, prostate cancer, lung cancer).
My tumor was unusual and had to be sent to UCLA’s tumor board for analysis. I had my very first PET scan that week. Before receiving the results I worried that my future was now limited. The questions were innumerable.
Would I survive the summer? Christmas felt like a long shot. What would life look like with a massive vertical wound that would someday become a scar on my belly? Would anyone ever want to date me again? Would employers want to take a chance on a young girl who might die from cancer soon? If my time was limited, what should I focus on?
My long term goals no longer mattered like they once did. How could I live a fulfilling life, not knowing if these weeks were the end of my life? I had always been a long term planner, taking actions with future me in mind, nevermind the present. Robbed of the certainty of my future, I was forced to make a monumental mindset shift.
After nearly a week of uncertainty and wearing a wound vacuum, I visited my assigned oncologist. He told me that the PET scan revealed no evidence of disease. This is the best news possible for cancer survivors, but it was hard for me to understand just how wonderful that was. I was, after all, newly inducted into the world of cancer and I still didn’t even know what kind I had had.
Eventually they determined it was clear cell sarcoma of the gastrointestinal tract. A research study conducted between 2004-2017 revealed only 53 cases of this cancer worldwide.
The statistics for clear cell sarcoma are grim. If you google it like I did, you will be faced with the phrase ‘poor prognosis.’ Five year survival is 56%; ten year is 33% and twenty year is 10%.
But now that I am in the one-third who makes it to this 10 year milestone my hope for old age is reignited. Yes, I need to remain vigilant. Especially because having radioactive glucose injected into my veins (procedure for PET scans) multiple times at a young age increases the odds for developing other cancers. But, now that I’m in the 10 year club there should only be a 23% chance that I perish before age 46. Much better than the 90% chance I once faced.
So today I celebrate this incredible milestone by indulging in the here and now. I took the day off work and filled it with activities that bring me immediate joy, writing is one of them.
Sunflowers are the symbol of sarcoma awareness. Photo by todd kent on Unsplash
Ten years has taught me so much and I have been incredibly fortunate, perhaps even blessed, to have such a magnificent quality of life. That is not always the case with cancer. Even those who survive 5 years are often undergoing treatments and battling relapses during that time.
I’ll be making a series of videos over the next month highlighting 10 perspective shifts that I have made since surviving cancer. I love to write about developing a resilient mindset, and those strategies are directly influenced by what I’ve learned as a cancer survivor. So, if you’d like, follow along on my YouTube channel.
I’ll also be raising money for the Sarcoma Foundation of America through the next month in hopes that my story can inspire newly diagnosed sarcoma patients and we can raise money for more research on these rare cancers that account for less than 1% of all cancers and mainly impact young adults. Check out my page on Raise Your Way to donate directly to my 10 year cancer free fund. My goal is to get 100 people to donate just $10. Of course, if you can donate more you are welcome to but $10 is all I ask. Thank you, everyone. Here’s to 10 more years!
As a career emergency manager and preparedness advocate it may strike you as odd, but I cannot stand community preparedness fairs. Many emergency services agencies have annual preparedness fairs and take great pride in the hours of logistical planning that go into it. They have traditionally been a key method of preparedness outreach. I certainly don’t discount these hours of hard work and the community traditions that have been built around these fairs. I just can’t stand them because I don’t believe it is an effective method for getting our key messages through to the public. I firmly believe we can make better use of our time and effort by trying new avenues of preparedness outreach.
Reason #1: Generic Information
The information that is being provided is too often a ‘one size fits all’ generic information pamphlet that takes the classic ‘get a kit, make a plan, stay informed’ and stamps that agency’s logo onto it. Information like this can be readily found online from any number of national organizations and has little added value from a local perspective. The brochures are often mass produced, with dangerous assumptions that every person who reads them comes from a similar background, has similar access to resources, and shares a common language. In some of the more diverse cities and counties, we do see information in multiple languages, which is a great start to solving this issue. But simply translating the same material into a different language is not going far enough. We need to create preparedness materials that are actually tailored to the cultures and perspectives of our target audiences.
Too often, the booths are staffed by volunteers, interns or hourly staff seeking overtime who aren’t overly enthusiastic about sharing the preparedness gospel. They may not even be familiar with the ins and outs of the different brochures and pamphlets that adorn their booths. Many times I have walked through preparedness fairs and seen booth staffers scrolling through their phones absently, seemingly counting down the hours until the event concludes so they can get back to their evening or weekend. Conversely, the most enthusiastic booths are inevitably staffed by vendors who are eager to tout their product and make a dollar, which can sometimes annoy attendees.
Reason #3: One Way Information Channel
Booth staffers provide information to community members. This is accomplished by handing them various flyers, explaining charts or graphics in the booth or by delivering the same canned preparedness information ad nauseam to each visitor. No wonder they aren’t enthusiastic, it’s downright boring to say the same thing over and over all day. Sometimes fairs also incorporate mini lectures from preparedness experts speaking on various topics. Lectures and brochures both share one important pitfall: they are one sided. They do not leave much room for dialogue or customization of the message. The knowledgeable person talks at the person who has come to learn and then sends them on their way, feeling moderately satisfied at having communicated the message. The problem is that while the attendee may have heard you, it’s unclear whether or not they actively listened or understood you.
Most preparedness fairs I’ve been to take an all hazards approach, where we try to cram all the preparedness information we possibly can into our booths and down the ears of visitors. This often results in an information overload, where the visitor quickly becomes overwhelmed and stops trying to absorb the information. The brochures are usually long, containing pages and pages of reference information. The visitor usually glances at it and then throws it into the bag with the rest of the brochures they’ve picked up.
Reason #5: No Follow Up
Many visitors have good intentions of reading the brochures, but how many of them ever do? It feels like they have accomplished something by attending the fair, enhancing their preparedness and receiving tons of information. But what good is a bunch of papers sitting in a bag in a closet? And if they do have time to read them when they get home, what if they have a question? Is there a clear, actionable next step that we are communicating to them? We tend to hold these fairs infrequently and rarely follow up with visitors to see if they have questions or have taken any action.
Reason #6: Preaching to the Choir
The type of person who chooses to attend the preparedness fair is usually someone who has some level of preparedness or understanding of hazards already. These people are typically civically engaged and active participants in other facets of their communities. The people who need the information the most are unlikely or unable to take the time to attend in the evening or weekend hours, when retail and service industry employees are often scheduled to work.
So what can we do to address these issues? If you are married to the idea of having a traditional preparedness fair, I think there are steps that can be taken to enhance the experience of your visitors. Get away from long, generic pamphlets. Focus on key messages that are locally applicable to your visitors. As much as you can, tailor information to the cultures and demographics where you will be holding the fair. Recruit enthusiastic people to staff the booths and provide them some training before the event. Set your expectation for them to facilitate two way dialogues with visitors, ensuring unique conversations with each person who visits. Introduce hands-on exhibits into the booths as much as possible, allowing visitors to interact with the material and incorporate tactile learning.
Radicalizing Community Preparedness
Instead of trying to make fairs better, why don’t we replace them with innovative, exciting events? It will take more creativity and may seem like a leap of faith to try something out of your comfort zone, but I promise that you will be rewarded with much greater enthusiasm and the knowledge that you have given your participants a truly educational and engaging experience. Radical preparedness events are a lot of work, but so are the logistics that go into planning a traditional fair.
I gave an EM Vision talk on this subject at the 2018 IAEM Conference in Grand Rapids. How can we create fun, non-traditional emergency preparedness events? In the framework I developed for innovative preparedness outreach, there are three core pieces that you must first define.
Start with a defined message.
There is so much to learn about preparedness and emergency procedures. We will have more success if we hone in on one subject at a time rather than trying to give everyone everything at once. Do you want to focus on your emergency notification? Evacuation? Hurricanes? Earthquakes? Preparedness Kits? Preparedness Plans? Pick the most pertinent topic for your community and go from there.
Select an interactive method.
People learn best when they engage directly with the material, ideally in a physical environment. This is where we can try to ‘game-ify’ preparedness and introduce some fun, good natured competition. When I was the Emergency Manager at Cal State Northridge, I designed two award-winning programs to help our students prepare. For one, I used a scavenger hunt concept and the other I used an escape room concept. There are many different routes you can go with this. Get creative–it can be a card game, murder mystery, a ‘create your own adventure’ story, or so many other things. The key is just that it has that interactive component.
Photo from CSUN’s 2016 Zombie Preparedness Scavenger Hunt
Utilize pop culture.
This is where you can make your event fun and attractive. By selecting a fun pop culture theme you will create a hook for your audience. It should be a theme that is similar to one you would use for a social party and/or fundraiser. At CSUN, I chose a zombie theme for one event and a 90’s theme for the other.
It may be scary and uncomfortable at first but I guarantee that the new buzz you generate around preparedness will be worth it! Visit my preparedness outreach page for more ideas.
Emergency Managers are experts in the art of compromise and consensus.
With infinite hazard scenarios to prepare for, including the emergence of cascading disasters as a reality, the job of an Emergency Manager is defined by our ability to adapt, pivot and re-prioritize based on the needs of the incident. In an Emergency Operations Center (EOC) in particular, the most effective Emergency Managers (EMs) are those who can “[get] highly specialized groups like doctors, police, wastewater management, economists, lawyers, politicians, etc. to come to a consensus on an emergency timetable,” according to Jason Vezina, the CEO of Prepared Canada Corp. What this means in practice, is the most effective EM is one who can synthesize multiple and disparate perspectives, and ensure any resulting solution is responsive to the needs of the emergency or operational period. It’s no surprise that what makes an exceptional EM are also the traits sought after in leadership positions – in both senior management and elected official contexts.
In order to move our discipline forward, consideration of our collective career growth and leadership opportunities is needed. We need to think beyond traditional goals of rising to leadership of state and national emergency management agencies. You may think that you have hit the ceiling in your current organization if you are in the most senior emergency management position. But perhaps there is room for local career growth into a broader leadership role that you haven’t yet considered.
As our profession matures, our backgrounds will be seen as less ‘niche’ and more essential to the core function of organizations – perfect platforms for leadership. We are so focused on the ever exciting world of disasters, many of us haven’t considered that we can (and should!) pursue promotional opportunities into the positions that oversee and dictate emergency management policy in our organizations. Leveraging our considerable experience and knowledge of best practises into policy positions will help to ensure that programming, budgets and departments incorporate an ‘EM’ perspective into corporate governance.
The payoff for our field will be huge if we can collectively make an effort to step into these positions and get the emergency management perspective integrated into boardroom meetings across the world. Rather than relying on our bosses to advocate for our programs, we can be the ones doing it directly if we become our bosses. Someone has to step into the leadership role, so why not emergency managers?
Generalists
You may worry that you don’t have the technical expertise or financial acumen to advance into a role that oversees multiple departments. However, anyone who advances to the highest level of leadership in organizations must generalize their knowledge. The more departments and programs under the purview of the leader, the less likely the person is to have intimate familiarity with all of them. Emergency managers already have an advantage in this regard because our work inherently familiarizes us with the different departments, functions and branches of our organizations. In order to develop a strong emergency plan and EOC team, we are already working with various departments across the organization. For continuity planning, we have honed in on the most essential functions of our organizations, we’ve learned who is responsible and the processes involved. These functions are not emergency management specific, however we have intimate knowledge of them that most other professionals do not possess.
Emergency managers are natural leaders. We run toward the fires rather than away from them. While others are shying away and melting down, we turn it on and rise to the challenge of crisis mode. When an emergency strikes our jurisdictions, we are the ones who elevate into the EOC Director roles (or advise the Directors in our roles as coordinators). Our colleagues and constituents turn to us for recommendations on next steps to handle the incident. They rely on us to be forward thinking and unwavering in times of crisis. Simply by stepping into this role as crisis leaders, we are demonstrating core competencies that are essential in everyday leadership. Many leaders would say that crises are some of the most challenging times to be in charge, and emergency managers are already leading during disasters.
Knowledge of Systems
We also have an understanding of the underlying societal systems that impact our organizations and our constituents. We are acutely aware of the factors that influence vulnerability and which segments of the community need the most support during disasters. Unsurprisingly, these populations tend to need the most support outside of crises as well. Disparities in access to resources, systemic racism, and generational poverty have huge impacts on who is disproportionately impacted during disaster. We are in tune with these and the cascade of negative impacts that can occur to these populations post-disaster. Oftentimes a simple promotion of personal preparedness is not enough to help, we need to address these inequities on a system wide level at the community level, and that work begins during blue skies. As an example, many Indigenous and remote communities face disproportionately greater impacts as a result of disasters. Our emergency management perspectives are a wonderful primer to these larger societal issues and chronic stressors that impact long term community health.
Emergency managers are relationship builders. Our jobs require us to motivate others without direct line authority as we must find creative ways to encourage compliance and participation across departmental lines. This is best accomplished through building strong working and interpersonal relationships with colleagues, establishing trust, and building knowledge of what skills, motivations, and hurdles are in their daily work. We know the importance of building connections prior to disasters, so we invest in our social fabric and take the time to get to know others in our organizations. These relationships that pay off in a big way during disasters can also reward us as we advance professionally since we have already established allies across and beyond our organizations. When we promote, our networks will allow us to transition smoothly into our new roles and strengthen the relationships we formed in emergency management.
We all know that the buck stops with the policy group (aka your organization’s elected leaders). While the advancement of emergency managers into VP or C-suite roles will be a huge boost to the discipline, emergency managers filling elected roles will truly instigate positive change. Emergency management provides a fantastic background for politics. Our missions are both altruistic and inspirational; life safety, preparedness and resilience are easy sells for public support. While a traditional law enforcement background can be politically divisive, emergency managers provide a more strategic and holistic approach to cultivating safe communities. The relationship skills that we use to motivate people to prepare for emergencies and strong networks we have built throughout our regions can be huge assets to launching a political campaign. Instead of strategizing on how we can get our elected officials to invest in disaster resilience, why not become the elected officials?
Recovery remains the murkiest phase of the disaster cycle. Unless you have experienced a significant disaster in your jurisdiction then you haven’t had an opportunity to practice and explore recovery concepts. Recovery does not have a well-defined beginning and end, therefore we tend to shy away from it and choose to focus our planning instead on the distinctive and adrenaline filled response phase.
FEMA has two primary recovery programs that provide disaster assistance: Public Assistance (for local and state governments) and Individual Assistance (for individuals / households). The first step in accessing these programs is a request from the Governor to the President to declare a Major Disaster. Once received, FEMA will review information about the disaster’s impacts.
The metrics they typically rely on include the estimated monetary value to public property (obtained through initial damage estimates submitted by the local jurisdiction), the number of private housing units that are damaged or destroyed and the number of these which are uninsured. Based on these numeric estimates, and the Preliminary Damage Assessment validation process, FEMA will make a recommendation to the President about granting a disaster declaration and which types of assistance should be activated. Sometimes, only one type of assistance will be granted initially, and then additional categories will get added as more information is collected and verified.
This view of recovery is narrow, focused only on numbers and physical damages. As I outlined in my recent article on the ripple effect of disasters, the true impacts of disaster tend to be much broader. These include interruption to work and loss of hourly wages, losses experienced by undocumented populations, loss of outbuildings that were used for primary residences, displacement of renters outside of the disaster zone, school closures and childcare impacts, health impacts related to poor air quality, economic impacts due to air quality related closures, and psychological impacts on the greater community.
When we begin to think about the true number of people who could be defined as disaster survivors, we see that the reach is much broader than who qualifies for FEMA’s Individual and Household Assistance program currently. Assuming that you live in a county that was included in a Major Disaster Declaration for which Individual Assistance was activated, you have to be able to prove that you lived in a disaster damaged residential structure, prove that you were uninsured or underinsured, and show evidence that a member of your household is a “US citizen, non-citizen national or qualified alien.”
As depicted in a recent NPR article on FEMA’s high denial rate for disaster assistance applications during the 2020 Oregon Wildfires, this is not an easy process. “During last year’s fire season in Oregon, FEMA didn’t approve roughly 70% of claims. That’s after FEMA filtered out applications it had deemed as potentially fraudulent. In California, FEMA didn’t approve 86% of claims.”
There is much room for error in the paperwork process and if the automated systems are unable to verify you along the way, your application will likely be denied. Of course, there is an appeal process but many who see the word ‘denied’ simply move on. Hassling with bureaucratic paperwork and jumping through hoops is the last thing that most disaster survivors want to do.
So if those who meet the currently narrow definition of survivors are experiencing their share of problems accessing aid, how do we go about creating a system that supports an expanded definition of disaster survivors?
Early 2018 meeting of Ventura’s Long Term Recovery Group
Involving Community Based Organizations
While government financial assistance can be extremely beneficial, it shouldn’t be relied upon as the only way to support individuals following disasters. That’s where non-profit organizations and community based organizations can step in to be incredibly important local assets. Case management efforts can be best coordinated by the formation of a Long Term Recovery Group (LTRG) for resource and information sharing. Following the series of disasters in 2017 and 2018 in Ventura County, the LTRG became a critical driver of recovery efforts. The group ensured that monetary grants provided by the American Red Cross, Tzu Chi, the Salvation Army and others were issued in a coordinated manner and helped survivors navigate the process of identifying and applying for all available aid.
One of the leading organizations in Ventura’s LTRG is the Ventura Community Foundation. Before my experience with the recovery, I was unaware of the role that such foundations can play after disaster. According to the Council on Foundations,
“Community foundations are grantmaking public charities that are dedicated to improving the lives of people in a defined local geographic area. They bring together the financial resources of individuals, families and businesses to support effective nonprofits in their communities.”
As a trusted fiduciary agent in the community, the Ventura Community Foundation has been able to provide both short and long term recovery grants to individuals and community based organizations impacted by disaster and also partner with grassroots organizations to amplify fundraising and giving efforts. This is a largely untapped resource for emergency managers, and a critical stakeholder to identify and bring to the table in pre-planning efforts. The mission of such organizations aligns closely with filling the gap between survivor needs and available assistance.
My experience and research on recovery has revealed that an effective recovery strategy is to expand our focus from individuals to the community. While financially supporting the most deeply impacted individuals is a critical component of recovery, there are many non-financial factors that can support survivor recovery too. One is having the ability to share their story, which is most effectively done through community healing events, such as fundraisers, vigils, and memorials that specifically recognize the hurt and trauma that disaster has caused. Effective case management staff, volunteers, emergency managers and any other representatives working with the survivors can also help meet this need simply by allowing space and time for survivors to share their experiences. It may take an extra hour out of a busy day, but as architects of community recovery we need to recognize and understand this need and build time into our agendas to allow it.
Another key factor in survivor recovery and post traumatic growth is feeling connected to something greater than themselves. Service opportunities allow survivors to give back and regain their agency, thus rewriting the narrative that might have painted them as ‘victims.’ Creating such opportunities alongside community events can be a huge booster in community resiliency and recovery. As much as possible, survivors need to find a place and mechanism to connect with one another, to hear each other, and to console each other. Local businesses and organizations can be huge assets in facilitating these opportunities.
When I gave my recovery presentation at the IAEM Encore conference last month, I was asked a really interesting question: If acres burned and homes destroyed don’t tell us the full story, what metrics should we be using to measure recovery? As I’ve considered this question, some immediate ideas drawn from the ripple effect come to mind. Perhaps we can look at economic statistics—jobs lost, hours lost (although how do you gather that data?), retail losses, tourism losses, agriculture losses, etc. And maybe we could measure through days that schools and other anchor community establishments are closed. Another possible metric could be the number of people seeking assistance through local non-profits. In Ventura County, a good indicator was the number of disaster related calls placed to their local 2-1-1 (help line for general questions on services, resources, and information in the county).
But the more I thought about the question, the more I realized that trying to find a quantitative method to measure recovery might be the wrong approach. Instead, maybe we need to try to measure it qualitatively. Numbers can only tell us so much. Metrics cannot convey the true human impact of disaster the way that survivor stories can.
To really illustrate true impacts, relief agencies need to understand what it was like to be there during the disaster and the lingering social, psychological, and economic impacts that survivors feel. Focusing on the direct financial impacts will only ever tell a sliver of the story. Let’s look instead toward ways to collect qualitative data—what are the themes of loss, hope and healing among survivor stories?
At the beginning of 2020, Ventura Community Foundation held a ‘Ted Talks’ style event where disaster grant recipients shared brief stories about the impact of the funds on their recovery. It was emotionally moving and hugely successful– benefactors left with a much deeper understanding of where their dollars were going and a strong motivation to continue giving. When survivor stories are published in media, they can also reveal losses and plight of the more ‘invisible’ members of the community.
In the recovery phase there is a fine line between making life better for disaster survivors and making life better in general. Often, disaster serves to illuminate pre-existing inequities and inadequacies in social systems. It’s hard to isolate needs that are related solely to the disaster and turn a blind eye to needs that also exist in blue skies. That is where recovery so closely blends into the mitigation phase of the cycle–what can we design, develop, and build back better so that the next incident doesn’t become a disaster?
This nexus between recovery and mitigation is the most fascinating to me personally, and the area where I think that our field has the most potential for growth. Here is the place where we can really show our value and embed our work with community development, economic development, urban planning, social advocacy, environmental justice, and other agencies who work on reducing social vulnerability every day. These may not be the first stakeholders we imagine when we think about whole community partnerships, but they are unequivocally important to engage during recovery. And as we all know, it’s better to build the relationships before the disaster hits.
Earlier this month I gave a presentation, Dynamics of Recovery: Navigating the Long Haul at the International Association of Emergency Managers Encore Conference. This was the first time the professional association had done a mid-year two-day virtual summit featuring follow up presentations by select speakers from last year’s conference. (You can view my 2020 presentation on Navigating the Transition from Response to Recovery here—it will be a few more months before I can release this month’s presentation.)
I was excited for the opportunity to expand on recovery after all the research I’ve been doing for my Ruin to Rebirth book project and the trends I’ve been seeing after recent disasters in California. One of the things I chose to focus on in this presentation was how we really need to broaden the definition of disaster survivors. When it comes to determining eligibility for disaster aid, FEMA tends to rely heavily on statistics of damaged / destroyed homes and the percentage of uninsured losses in a community. The need for simple metrics is understandable when you must make comparisons between communities to determine the areas of greatest need. However, this approach is a drastic oversimplification of the impact disasters have on communities. In this article I will discuss the ripple effect of California’s wildfires as background for an upcoming article on new ideas for measuring recovery and how we can broaden the definition of disaster survivors.
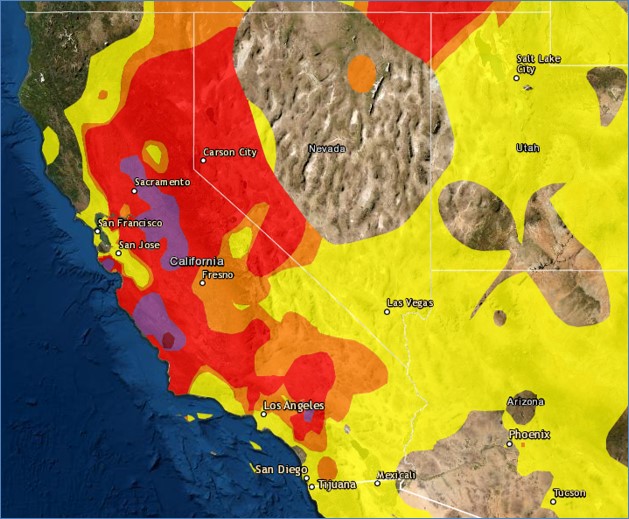
A screenshot of California’s air quality map on 8/20/20 captured from Purple Air.
Smoke’s Influence on Air Quality
When discussing wildfires, the influence of smoke on air quality is a key issue that drives disaster impacts way beyond the burn area. While the direct physical impacts of flames are limited even in large fires, smoke quickly becomes a regional or even statewide affair. In California’s 2020 wildfires air quality impacts were observed hundreds of miles from the burn areas for nearly an entire month. When air quality is poor it ignites a domino effect of negative consequences for industries—prompting closures at schools, outdoor retail, recreation, and tourism, and placing severe limitations on agriculture, construction, and landscaping.
Poor air quality has also been linked to dire health impacts. During widespread smoke incidents, both emergency room visits and deaths of elderly people increase dramatically. While the official fatality count for the 2020 wildfires is 26, a Stanford study estimates that this number could be up to 50 times higher—up to 3,000–when smoke impacts are factored into the equation. “These are hidden deaths. These are people who were probably already sick but for whom air pollution made them even sicker,” Marshall Burke, Deputy Director of Stanford’s Center on Food Security and the Environment told the San Jose Mercury News.
With chronic respiratory disease such as asthma on the rise in recent years, likely due to ambient air pollution, this is especially troubling for the health consequences that prolonged and frequent wildfires could have on younger populations too. The 2020 wildfires also coincided with the COVID-19 pandemic, meaning that there was an even greater vulnerable population with compromised respiratory systems due to the disease.
2017 Thomas Fire: Economic Impacts
As you might remember from previous articles, I was heavily involved in the response and recovery to the Thomas Fire in Ventura County through my role with CalOES. So I’d like to share some impacts that the Thomas Fire had on Ventura County to illustrate how deeply the community was disrupted beyond the modest 1,000 or so homes that were lost. These social and economic impacts begin to help us understand the magnitude of the ripple throughout the community, much of it instigated by smoke.
The Thomas Fire began on December 4th, the height of the holiday shopping season for many of Ventura’s small retail businesses. In Southern California’s ideal coastal climate, many businesses are located in outdoor shopping malls that were forced to close due to poor air quality during a critical time period in the shopping season. It was estimated that retailers in the impacted and adjacent areas would lose 20% of their annual revenue for 2017 and continue to feel losses into 2018 due to the fire.
Agriculture makes up a large percentage of Ventura’s local economy. As smoke permeated the valleys below the flame engulfed mountains, it was unsafe for outdoor farmwork to continue and many of the community’s most vulnerable were out of work during the holiday season. No workers meant no crops and thus agriculture suffered too. Crops were also directly impacted by the heat of the fire. Avocados are one of the top 10 agricultural exports in Ventura’s $2.2 billion dollar industry. The 2017 yield for avocados was decimated by the fire. But the impacts of the high heat were not limited to the current fruits, as it also caused a massive die off of the avocado trees, which would destroy business for years to come.
Tourism is another major industry in Ventura county. The picturesque location linking the Pacific Ocean with agricultural plains and oak covered hillsides makes for a perfect getaway backdrop. The Ojai Valley is reliant on tourism with about 31% of all jobs in that industry. Nestled in the rolling hills it is an ideal spot for retreats–for both business and pleasure. The Thomas Fire caused the Ojai Valley Inn, one of the major employers and economic drivers for the community, to close for two weeks as most of the Ojai Valley was evacuated when it was entirely surrounded by fire. Smaller hotels and businesses in Ojai were also closed. These closures caused many hospitality employees to lose hours or suffer unpaid weeks off during a time when most were reliant on their paychecks to give their families a good holiday season.
In all three of these industries, the majority of workers are hourly. Due to the uncertainty of the crisis, most employers were simply reducing hours rather than laying workers off, thus the true impact on jobs remains unknown since it is not reflected in unemployment data. This also made it difficult for workers to plan financially or access unemployment benefits since they were not technically unemployed.
School Closures
Due to air quality issues in the Thomas Fire, most of the schools in Eastern Ventura County were closed for two weeks in December prior to their holiday break. As the nation has seen during the COVID-19 crisis, school closures have massive ripple effects in a community. When children are out of school, many parents are forced to stay home from work–often in sectors that are not well equipped for telework or in industries where they do not have sick or vacation time benefits to use. This puts additional financial strain and mental stress on families who are forced to adapt to a lifestyle where everyone is at home and parents are unable to earn income or work productively. Many low income families are also reliant on school lunches so school closures can increase hunger and food insecurity in the community.
During the 2020 wildfires, I was managing the California State University system’s response. Over the span of August to September, we had seven campuses close for at least one business day due to poor air quality. We also had at least 26 members of our CSU campus communities lose their homes due to the wildfire. Power outages, evacuations, and closures also influenced the ability of students and faculty to participate in online courses, which made up most of our academic offerings at the time due to the pandemic.
Prior to the fire, Ventura had already been experiencing a housing crisis. Rates of homelessness were on the rise due to increasing rents and plummeting vacancy rates. Ventura County was in the top ten least affordable housing markets in the nation and only about a quarter of the County’s population could afford a median priced home. The vacancy rate in Ojai was less than one percent and Ventura’s was less than 2%. So even if you were in that lucky 25% who could afford to own a home, they were incredibly difficult to come by.
The fire only exacerbated the housing crisis in Ventura. While over 900 housing units were destroyed, the County knew unofficially that many of these units housed multiple families, sharing space to alleviate the high cost of rent. There were also over 200 outbuildings destroyed. Although FEMA would not count these as homes in the certified count, it was known that many of them were occupied by extremely low income farm workers. Since they were not technically residential units these people would not have access to many of the benefits that other disaster survivors would.
Another way that the housing market shifted after the fire was through the displacement of renters. While the fire itself destroyed many large beautiful homes in the hills, renters in Ventura city came to bear the burden of seeking new housing. This was because homeowners in the destroyed neighborhoods owned more than one property. So, when their primary residences were destroyed, these landlords relocated to their rental units while rebuilding their homes. This meant that renters who had been paying month to month were now given notice and had to join the incredibly difficult hunt for housing in Ventura. They were an entirely untrackable population who were deeply impacted by the fire, having lost their place of residence but would have no access to any survivor benefits and would simply be on their own to fight for housing.
Looking Forward
To really understand this dynamic, complex, and lengthy phase of the disaster cycle, we need to broaden our perspective and consider the far-reaching impacts of disaster on our communities. In my next article, I will discuss new ideas for measuring recovery that go beyond the simple metrics of acres burned and homes lost.
As large organizations begin to repopulate following extended remote work due to COVID-19, many employees are questioning why it is necessary to return to the daily office environment. Telework has been a popular option for people, allowing them to spend more time with family and pets yet avoid time consuming commutes. Yet there is some resistance to a permanent telework environment, with managers questioning productivity and fearing the erosion of team bonding.
Some organizations are allowing for flexible, hybrid schedules that allow a sort of compromise. Where do emergency managers fall in the spectrum of employees that can perform their jobs effectively from home? If your organization allows a choice, should you take the opportunity to work from home or will it hurt your emergency management program?
As we see a shift toward continued remote work across progressive organizations, these are critical questions for current emergency managers who have enjoyed the work from home life as well as those considering emergency management careers.
Remote Response Coordination
As I wrote about during the height of the pandemic, emergency management coordination can be done remotely. With an array of technological tools at our fingertips, there is no reason that we can’t continue to practice remote coordination in a post-pandemic environment. Unlike our partners in police, fire or healthcare, our work does not involve physically interacting with the community. We would do well to keep our virtual EOC plans well exercised, because an emergency may very well happen while employees are at home. Virtual coordination can occur immediately, you don’t have to wait for people to drive into the EOC when roads may be compromised and precious minutes matter. Especially if a portion of your organization’s workforce will become permanently remote, this practice will be more crucial than ever.
It is ultimately very important for the emergency management program to mirror the organization’s culture. To reach our goal of embedding resilience in the DNA of our organizations, we must be willing to mold our programs to meet the existing needs of the people. If most employees in your organization will be in the office most days, it’s probably best for you to develop in person training, programming, and plans for in person EOC activations. If most of your organization will continue with remote work, then there is no reason that you should feel obligated to go into the office to ‘prove’ that you are essential. You should focus your time on developing online training and programming. While remote emergency response coordination can be done effectively, I have found a hybrid model to be challenging. If most of your EOC is in person but a handful of folks are remote, chances are those people are going to be left out of important conversations and will end up missing out on information they need.
Balance of Workload
One of the reasons I enjoy my career in Emergency Management is that it is not ‘just a desk job.’ After years of working in other office occupations, I dreaded the ‘butts in chairs’ model of being chained to a desk from 8-5 every week day for the rest of my life. I have always enjoyed the variety of our work—there is a good balance of independent desk work (i.e. writing and reviewing plans / procedures, designing training materials & presentations, using information management skills to track program analytics) and people work (delivering trainings / exercises, participating in community preparedness events, conducting planning meetings and/or site assessments). Both the introvert and extrovert skillsets are necessary, and they help to keep the job exciting. This is one of the reasons why I would argue that almost every emergency manager should work level of a hybrid schedule. I am personally very productive in my home environment where I can get to work quickly and without interruptions. But I very much miss the amplified value of delivering training in person and developing relationships with key partners. Zoom is a much better substitute for these relationship building activities than conference calls, but it will never provide quite the same level of familiarity as an in-person exchange.
One other consideration regarding workload is whether you have a team or if you are the only emergency manager for your jurisdiction. With a team, a hybrid work model can balance out concerns about having a constant emergency management physical presence just in case a disaster strikes. This can be done through alternating days of the week, or by having a ‘duty team’ alternating in person work weeks.
This tried and true mantra of emergency management stands steadfast. Whether you are doing it in the flesh or through technology, you must prioritize effective working relationships with personnel in your organization and fellow emergency managers. The best way to build relationships and develop trust is in person. Going out to coffee, lunch or happy hour with colleagues can reinforce these relationships and is tough to do over zoom. As public health measures allow, it’s a good time to reconnect and build these interpersonal relationships. When it comes to meetings, I do think that the frequency in which we meet can be reduced from pre-pandemic times. Save your in-person meetings for longer events—workshops, conferences, or key training events that will include some element of socializing are the best use of your in-person time. Regular, business-oriented meetings can be more efficiently conducted over technology. If your work culture is shifting to mostly remote, schedule check in one-on-one zoom calls with colleagues and send personal emails periodically to replace some of the water cooler chat that you may have conducted in pre-pandemic times.
Geography of Your Jurisdiction
One factor to consider is the size and geography of your jurisdiction. As emergency managers, we have responsibility for being familiar with our areas and the various hazards associated with them. When I was working at a university, I made sure to get out of my office and visit other parts of campus so that I could learn the buildings and programs—even if it was just taking a walk on my lunch hour. It was important to get a feel for how many people were in each area at different times of day. While at the Southern Region of CalOES, I loved my many ‘field days’ which were devoted to building relationships by visiting counties / cities at their own EOC’s, conducting wildfire damage reconnaissance, and performing hazard assessments by physically acquainting myself with the situation. The need for periodic fieldwork won’t go away if you are working mostly remotely. Make sure to consider these needs when planning your schedule. If your jurisdiction covers a large geographical area, Zoom and other video conferencing technologies will continue to be good tools to maintain stakeholder relationships without forcing people to drive one hour each way regularly for a one-hour meeting.
There are many societal benefits that can come from a conversion to mainly remote work besides employee satisfaction. Organizations continuing permanent remote work can save on the costs associated with utilities and facility space if it is leased or rented. The environmental burden of thousands of fossil fueled vehicles idling on freeways can be reduced if employees do not need to make synchronous long commutes. People do not have to endure long hours of sitting in traffic, which is known to raise stress levels. Instead, they can use the extra time in the day to promote their health through exercise, meal preparation or relaxation. From an emergency management perspective it also reduces the ‘in between time’ when the workforce is not at their homes or their offices—this would be the worst time for a large earthquake to strike, since it would be incredibly difficult to account for everyone and to get your EOC team together.
In Conclusion
There are a several factors to consider when planning for the ideal post-pandemic emergency management work model. At the end of the day emergency managers must remain nimble and adaptable. Unless you are a consultant who performs very technical emergency management work without a need for sustaining relationships, you should plan for some degree of in person working days. For those with large geographic areas, remote relationship building, and coordination will continue to be paramount. It is important to tailor your program to meet the needs of your organization’s culture, which may be undergoing significant post-pandemic shifts. Now is a very important time to tune in to your organization’s plans, the desires of your colleagues, and talk with your peers about their long-term work models.